



Protocol:
In this cohort study, the data collection will be based on six methods (physical examinations, questionnaires, tests, clinical data, biological samples, and survey of living environment) that complement each other in order to cover multiple aspects of determinants of health and health outcomes. We will use standardised questionnaires and protocol applied by birth cohorts in Europe, which will facilitate publication of results of our analyses in leading international journals and also will ultimately make it possible for pooling data and conducting joint-analyses with European cohorts in future.
Because of the costs and practical reasons, it will not feasible to collect all the desired data (as listed below) for all planned mother-child pairs for the cohort. We will therefore use a novel 3-level nested design:
A. General cohort:
a survey of 150,000 pregnant women across all designed centres for which we will collect data on:
- Physical examination
- Questionnaires
- Tests
- Clinical data
- Biological samples
- Living environment
B. Broad sub-cohort:
10,000-15,000 pregnant women selected from the general cohort in large centres for which in addition to the data that we collect for the general cohort, we will collect data on
- Tests
- Biological samples
C. Omics sub-cohort:
5000-7000 pregnant women selected from the broad sub-cohort for which in addition to the data that we collect for the general cohort and broad sub-cohort, we will collect data on
- Tests
- Biological samples:
- Living environment
Conceptual framework:
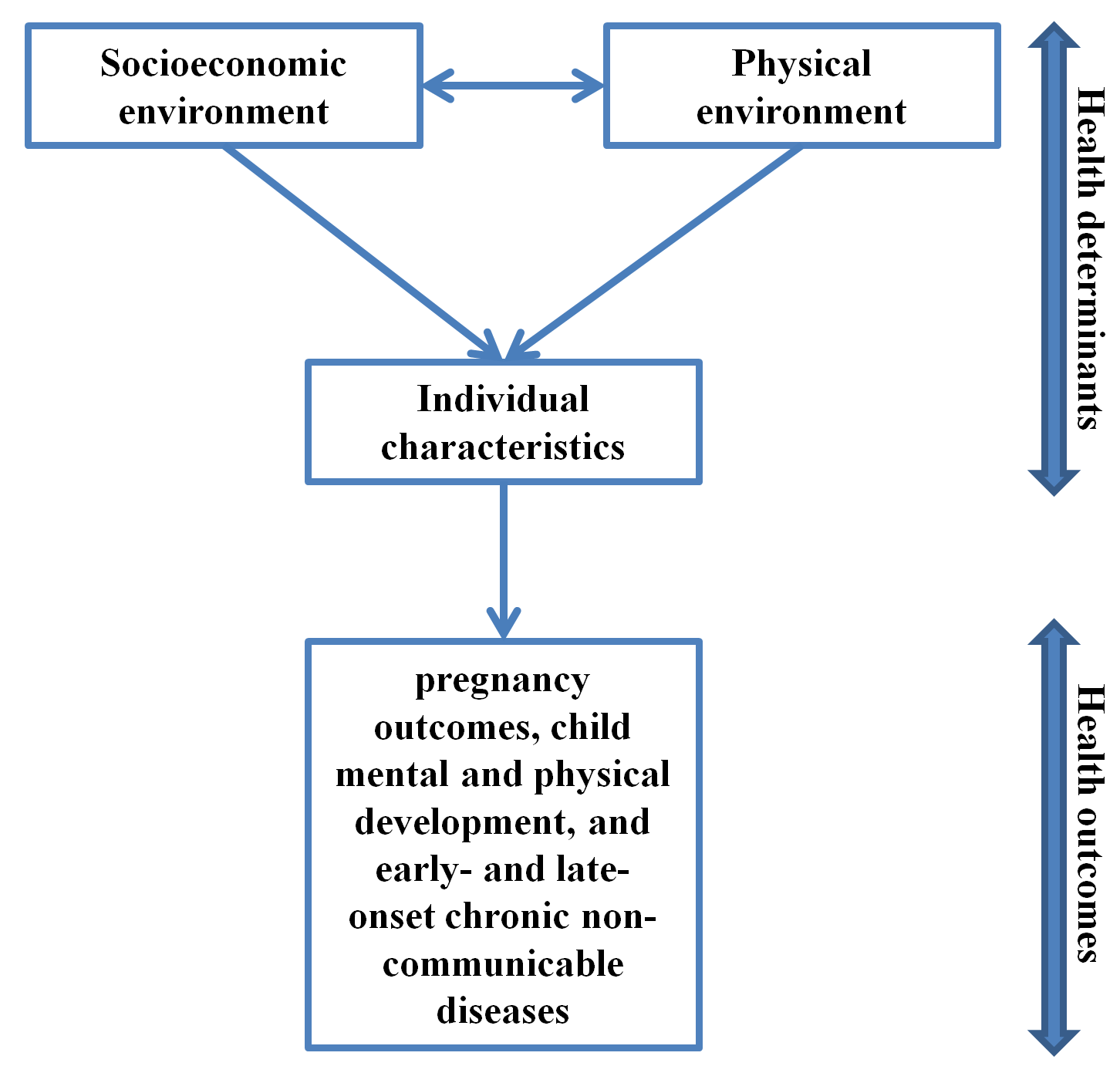
We will collect data on both “determinants of health” and “health outcomes”. Our evaluation of the “determinants of health” will encompass all three domains defined by WHO: socioeconomic environment, physical environment, and individual characteristics and behaviours (Figure 1). As described below, for each domain we will collect data on a number of sub-domains which, based on available literature, can be relevant to pregnancy outcomes, child mental and physical development, and early- and late-onset chronic non-communicable diseases.
Figure 1. Health determinants and outcomes covered by the project.
Study setting:
The PERSIAN birth cohort will be established in a number of centres for the PERSIAN adult birth cohort and will make use of already available infrastructures for these cohorts.
The pilot phase will be conducted in Isfahan and Yazd. A description of basic characteristics of these centres is presented inthe table below:
Recruitment of participants
We will select a combination of public and private healthcare providers in order to ensure they represent the ethnic and socioeconomic distribution in the underlying population. Pregnant women will be approached during their first pregnancy visit (at the end of first trimester) to these centres. Those consenting will be recruited if they have Iranian nationality, reside in the catchment area of the study centre, have a singleton pregnancy, give birth in the reference hospital, have not used assisted reproductive techniques, and do not have any communication problem. The high rate of Caesarean section in Iran will provide PERSIAN birth cohort a unique opportunity to evaluate the short- and long-term health effects of Caesarean section. The child’s biological father will be also invited to participate in the study at the first pregnancy visit (directly if attending the visit and indirectly through letters if they are not attending the visit).
Data collection:
Data collection will involve mother, father, and the child in the following five consecutive phases:
- Phase 1: Periconception till birth
- Phase 2: Infancy (0-2 years)
- Phase 3: Childhood (3-11 years)
- Phase 4: Adolescence (12-18 years)
- Phase 5: Adulthood (19-30 years)
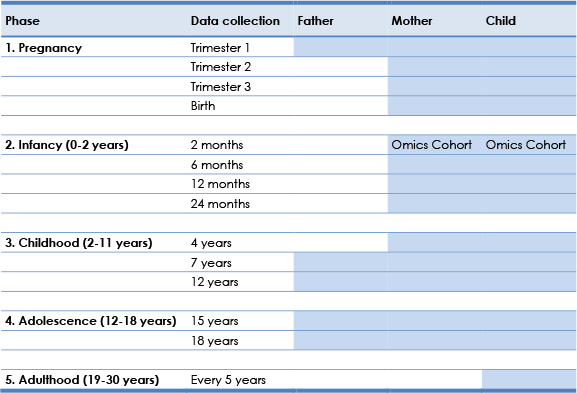
A description of data collection timeframe is presented in Table 1.
Table 1. The phases and time points of data collection.
Health determinants and outcomes:
Data on a wide range of determinants of health and outcomes will be collected as detailed in Table 2.
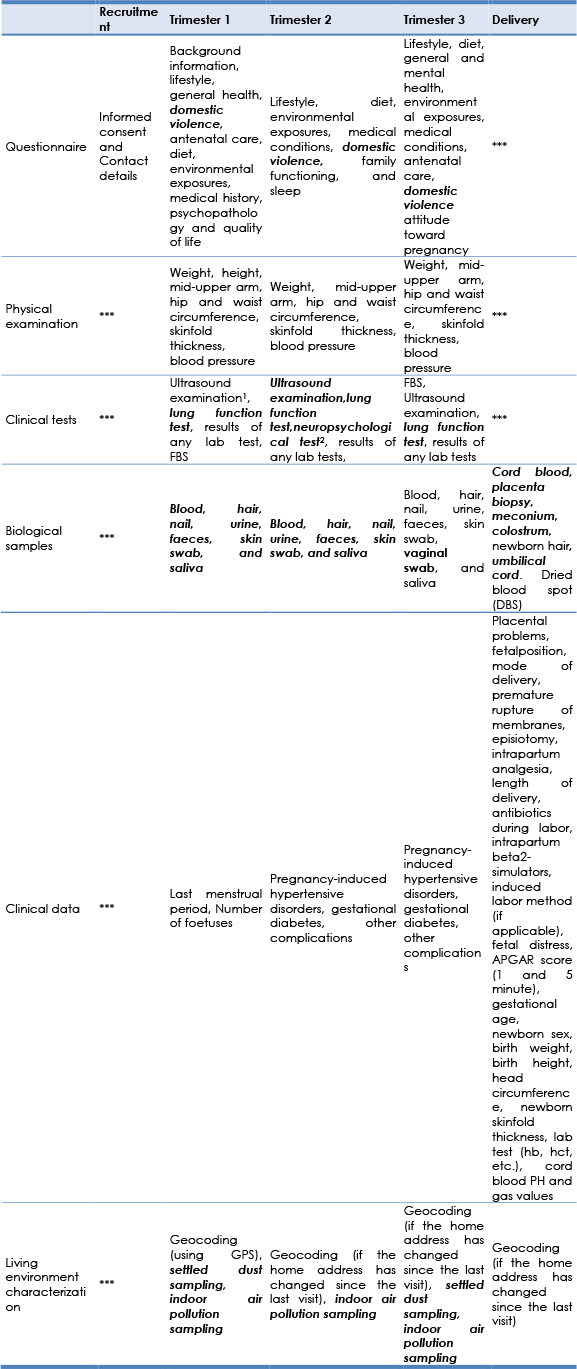
Table 2. Description of planned collected data.

1 Smoking, alcohol consumption, recreational drug use
2 Including syphilis, toxoplasmosis, rubella, cytomegalovirus infection, herpes simplex, hepatitis B & C, HIV, urinary track infections, vaginal GBS colonisation, and chorioamnionitis.
3 Including placenta praevia and placenta abruption
4 City and healthcare centre (or home)
5 Normal vaginal delivery, assisted vaginal delivery (induction, forceps, vacuum, amniotomy, and/or episiotomy), and caesarean section (elective, emergent, or during labour)
6 Stillbirth, maternal mortality, prolonged labour, haemorrhage, uterine atony, foetal distress, umbilical cord prolapse/compression, nuchal Cord, and meconium aspiration.
7 Analgesics/anaesthetics, antibiotics, beta2-simulators
8 Including length of gestation (days) and premature rupture of membranes
9 Birth weight, length, head circumference, and indications of IUGR.
10 Height, weight, skinfold, waist circumference, hip circumference, and bioelectrical impedance analysis
11 Lung function test (TLC, FEV1, FVC, FEV1/FVC)
12 Blood pressure and cardiac output
13 Iron-deficiency anaemia and G6PD deficiency
Data collection methods:
Our vision is to secure the potentials for international collaborations and taking part in consortia of European and regional cohorts in future international research projects. Accordingly, we will apply standardised questionnaires and protocols that are tailored and, where available, validated for the Iranian population and at the same time applied by established birth cohorts in Europe (e.g. INMA, MOBA, BiB, Generation R, and ALSPAC). This approach can also facilitate publication of the findings of PERSIAN cohort in high impact international journals.
The data collection will be based on the following methods that complement each other in order to cover multiple aspects of determinants of health and health outcomes:
- Computerized questionnaires
- Biological samples
- Physical examinations
- Clinical tests
- Hospital records
- Survey of living environment
Measures to ensure high turnout during follow-ups
At the time of recruitment, we will obtain the following information in order to achieve multiple was to access the percipients: XXX
To arrange the follow-up visit, first we will send a letter to participants one month before their follow-up time, informing them about the upcoming follow-up and what that follow-up will include (e.g. topics of questionnaires, types of biological samples, clinical exams, etc). Two weeks prior to the visit, the participants will be contacted over the phone and will be asked about their time availability to confirm the time and the date for the visit. One week and one day before the visit, the participants will be sent reminder text messages.
Data collection in Phase 1:
Phase 1 Data collection design
Because of the costs and practical reasons, it will not feasible to collect all the desired data (as listed below) for all planned mother-child pairs in the cohort. Therefore, additional detailed data collection will be conducted in a selected subgroup of children and their parents from foetal life onwards.
A. General cohort:
a survey of 20,000 pregnant women across all designed centres for which we will collect data on:
- Physical examination (as described below)
- Questionnaires (as described below)
- Clinical tests (mother):
- Fasting blood sugar
- Ultrasound examination (Twice at first and third trimesters to assess foetal growth and gestational age)
- Clinical data (as described below)
- Biological samples
- Mother
- Blood (once)
- Urine (once)
- Hair (once)
- Nail (once)
- Skin swab (once)
- Faeces (once)
- Father
- Saliva (once)
- Newborn
- Hair (once)
- Dried blood spot (once)
- Meconium
- Mother
- Living environment
- Geocoded home addresses
- Home characteristics (as described below)
B. Omics sub-cohort:
5000-7000 pregnant women selected from the general cohort for which in addition to the data mentioned above for the general cohort, we will collect data on
- Clinical tests (mother)
- Ultrasound examination (once each trimester to access foetal growth (the second trimester examination should occur around week 20), brain development and cerebral ventricular volumes, fetal umbilical artery and the middle and anterior cerebral arteries, and placental echogenicity and perfusion)
- Neuropsychological tests (once)
- Biological samples:
- Mother
- Blood (once per trimester and once at delivery)
- Urine (once per trimester)
- Faeces (once per trimester)
- Skin swab (once)
- Colostrum
- Saliva (once per trimester)
- Vaginal swab (once at the third trimester)
- Newborn
- Cord blood
- Placenta
- Umbilical cord
- Father
- Skin swab
- Living environment
- Home indoor environment sampling (as described below)
- Home surrounding environment (as described below)
- Settled dust (Twice at 1st and 3rd trimesters)
- Mother
Phase 1 data collection methods
We will collect data from the mother, father, and the child using questionnaires, biological samples, physical examinations, clinical tests, hospital records, and survey of the living environment as detailed in table 3. The tasks planned for each Phase 1 visit are detailed in Table 4. Table 5 describes the information planned to be collected through questionnaires. Table 6 details methods that will be applied to assess exposure to environmental factors.
Data collection for the mothers and children using questionnaires, biological samples, physical examinations, and clinical tests will be conducted in the PERSIAN cohort centres. In each PERSIAN cohort centre, a team consisting of a general practitioner, a nurse, and a psychologist will conduct face-to-face interviews with participants to fill the questionnaires (psychologist), physical examinations (GP), and obtain and process biological samples (nurse). Participants in phase 1 are pregnant women and their husbands. In phase 2, participants will be mother-child pairs and the father of the child who were enrolled in phase 1. At their visits to the PERSIAN cohort centres, the mothers will be asked to take self-administered questionnaires for the fathers and return the filled questionnaires in their next visit. The answers will be checked by PERSIAN cohort stuff and if the answers to some questions were missing, the participants will be called on the phone and will be asked to answer those questions (for details on the follow-up protocol see section...).
We will assign two full-time midwives to each participating hospital in order to obtain data from hospital records of the participants and collect biological samples at the time of birth. The home visits (for geocoding and characterizing the home environment) will be carried out by an environmental health technician. To enhance the compliance among the participants, it is advisable to recruit female staffs for all the aforementioned positions.
Table 3. Data collection methods and timeline during Phase 1.
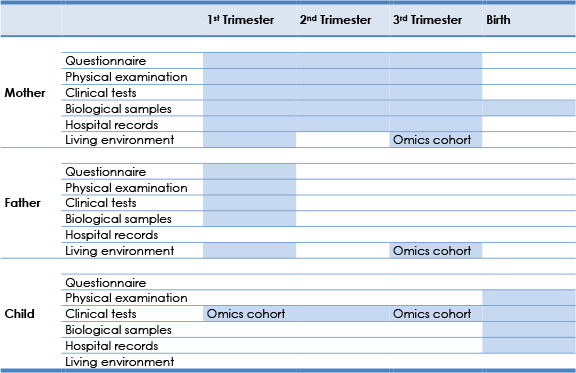
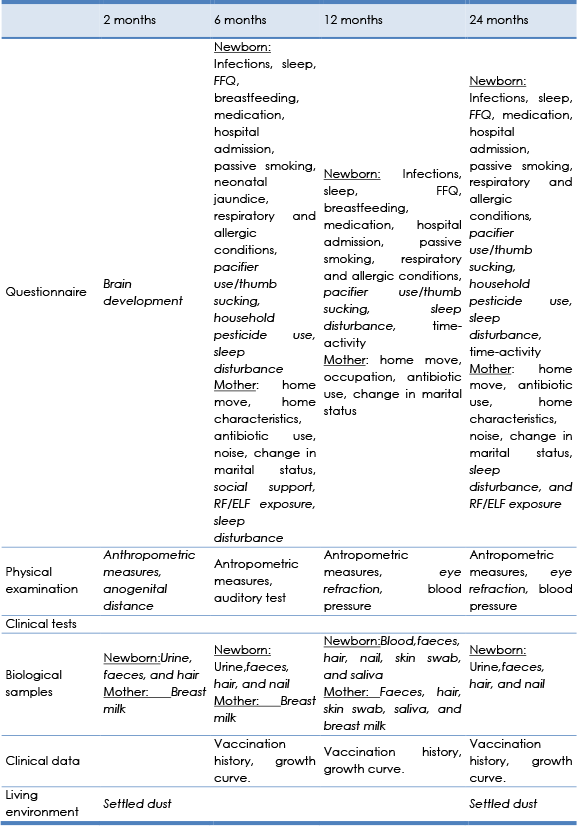
Table 4. Tasks during each Phase 1 visits. Tasks with underlined fonts apply to both father and mother, those in bold fonts apply to child, and those in normal fonts only apply to mothers.
1 To determine gestational age, to monitor foetal growth, to determine mental development, and to evaluate placental echogenecity and perfusion
2 working memory, IQ, verbal skills
Table 5. Description of questionnaires used in Phase 1.
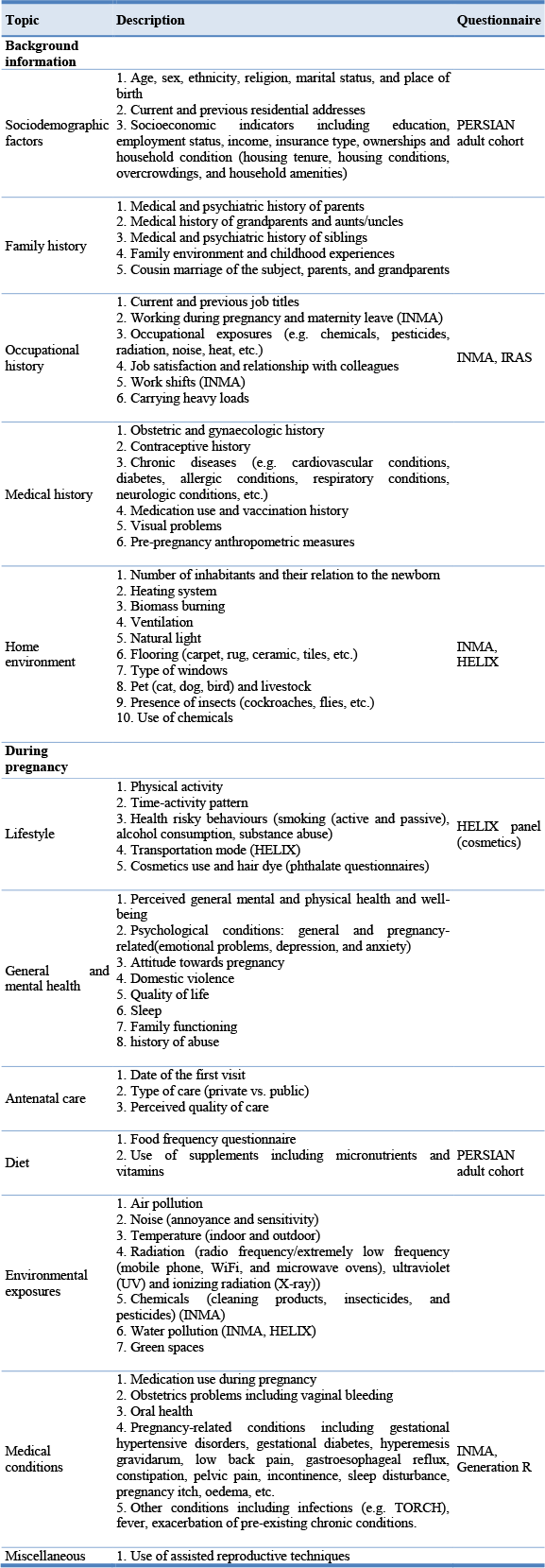
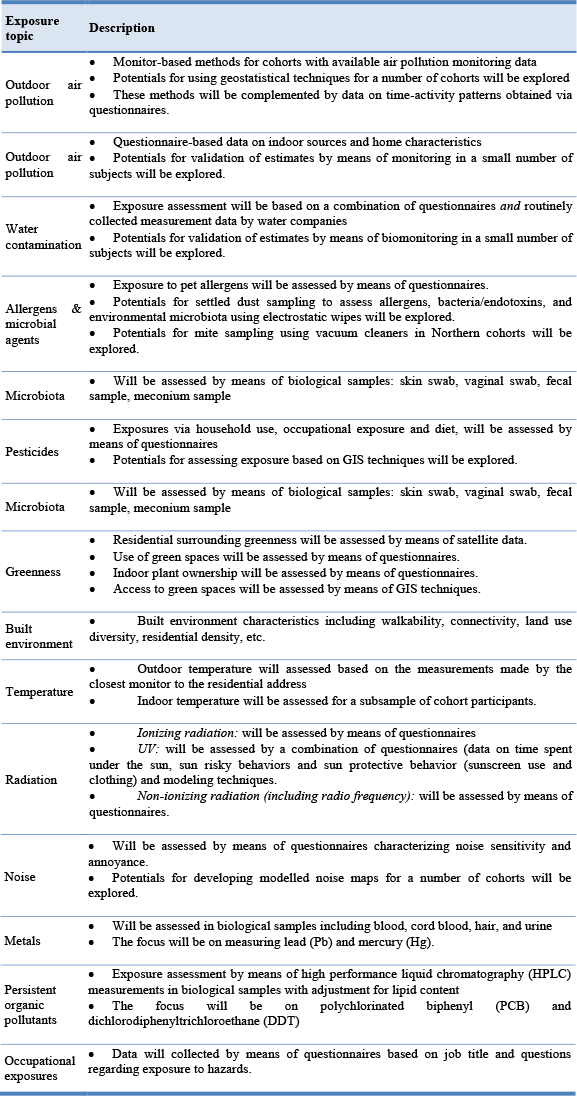
Table 6. Assessment of exposure to environmental factors.
Data collection in Phase 2:
Phase 2 Data collection design
In Phase 2, we will follow pilot study participants and Phase 1 general and omics cohorts:
A. General cohort:
for which we will collect data on:
- Physical examination (child)
- Anthropometric measures
- Height, weight, and head circumference: every two months from log-book
- Skinfold thickness (triceps and sub-scapular), mid-upper arm circumference, waist circumference, and hip circumference: three times at 6, 12, and 24 months
- Motor development (WHO milestone questionnaire)
- Blood pressure (twice at 12 and 24 months)
- Auditory test (once at 6 month)
- Anthropometric measures
- Questionnaires (child)
- Child
- Infections (three times at 6, 12, and 24 months)
- Time-activity (twice at 12 and 24 months)
- Asthma and wheeze (6, 12, and 24 months)
- Allergy, eczema, and food allergy (6, 12, and 24 months)
- Diet (breastfeeding, multivitamin/supplements, etc.) (three times at 6, 12, and 24 months)
- Medication (three times at 6, 12, and 24 months)
- Hospital admissions (three times at 6, 12, and 24 months)
- Passive smoking (three times at 6, 12, and 24 months)
- Neonatal jaundice (Once at 6 months)
- Mother
- Mental health (depression, anxiety, life events)
- Occupation/employment (mother and father) (Once at 12 months)
- Home move (three times at 6, 12, and 24 months)
- Home characteristics: presence of pets and animals (twice at 6 and 24 months)
- Antibiotic use (three times at 6, 12, and 24 months)
- Noise (Twice at 6 and 24 months)
- Change in marital status (three times at 6, 12, and 24 months)
- Child
- Health care and clinical data (child)
- Vaccination history: every two months from the log-book
- Growth curve: every two months from the log-book
- Biological samples
- Child
- Urine (twice at 6 and 24 months)
- Dried blood spot
B. Omics sub-cohort:
- Physical examination (child)
- Anthropometric measures: Skinfold thickness (triceps and sub-scapular), mid-upper arm circumference, waist circumference, and hip circumference (an extra time at 2 months)
- Eye refraction (twice at 12 and 24 months)
- Anogenital distance (Once at 2 months)
- Questionnaires
- Child
- FFQ (three time at 6, 12, and 24 months)
- Pacifier use/thumb sucking (6, 12, and 24 months)
- Household pesticide use (6 and 24 months)
- BPA/Phthalates
- Sleep disturbance (6, 12, and 24 months)
- RF/ELF exposure (twice at 6 and 24 months)
- Mother
- Child and mother relationship (once at 6 months)
- Social support (once at 6 months)
- RF/ELF exposure(twice at 6 and 24 months)
- Sleep disturbance (three times at 6 and 24 months)
- Contraceptive use (twice at 12 and 24 months)
- Menstruation (twice at 12 and 24 months)
- Father
- Mental health (depression, anxiety, life events)
- Sleep
- Child
- Clinical tests
- Structural MRI and resting state fMRI and Diffusion tensor imaging (DTI) MRI for a subset of 100 children
- Biological samples
- Child
- Blood (once at 12 months)
- Urine (four times at 2, 6, 12, and 24 months)
- Faeces (four times at 2, 6, 12, and 24 months)
- Hair (four times at 2, 6, 12, and 24 months)
- Nail (three times at 6, 12, and 24 months)
- Skin swab (12 months)
- Saliva (12 months)
- Mother
- Faeces (12 months)
- Skin swab (12 months)
- Saliva (6 and 12 months)
- Breast milk (two times at 2 and 6 months)
- Child
- Living environment
- Settled dust (Twice at 2 and 24 months)
Phase 2 data collection methods
We will collect data from the mother, father, and the child using questionnaires, biological samples, physical examinations, clinical tests, hospital records, and survey of the living environment as detailed in table 7. The tasks planned for each Phase 2 visit are detailed in Table 8. Table 9 describes the information planned to be collected through questionnaires.
Table 7. Data collection methods and timeline during Phase 2.
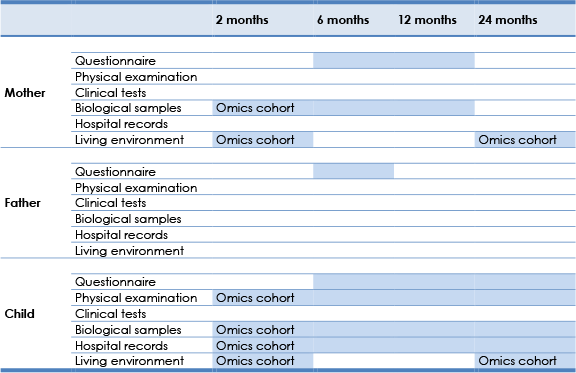
Table 8. Tasks during each Phase 2 visits. Tasks with underlined fonts apply to both father and mother, those in bold fonts apply to child, and those in normal fonts only apply to mothers. (Tasks in bold fonts are carried out only for Omics Cohort)
Quality control:
Critical to the success of the study is high quality data. Quality control procedures will happen in three stages of the study: during preparation for data collection, during the process of data collection, and after data collection is finished. Before starting data collection, study staff will have training sessions. During data collection, reports of summary statistics regarding questionnaire and visit data collection items are necessary to ensure form completion, appropriate use of skip logics and valid ranges. During and after the completion of data collection, data are quality controlled in real-time through the use of range limits and prompts for missing.
Timetable
Pilot study and Phases 1-2

Ethical considerations:
Participation in the surveys is voluntary and participants have the right to withdraw from study at any time. Potential participants will be provided information about the study, measurements to be conducted and possible risks they may pose in written and oral formats. Those who decide to participate, will sign the informed consent form before examinations start. Depending on the requirements of national Ethics Committee, the informed consent may include separate points for questionnaires, physical measurements, biological sample collection, and DNA testing, or may provide general consent for all included measures. All PERSIAN Cohort activities will be carried out according to existing guidance in ethics as indicated in the Universal Declaration on Bioethics and Human Rights adopted by UNESCO (19/10/2005).
This project concerns the collection of personal information from the participants and biological samples including blood, urine, hair, nail, faeces, skin flora, deciduous teeth, milk, meconium, saliva, cord blood, and placenta. PERSIAN birth cohort will ensure standardized protocols are used and will collect biological samples. The collection of the biological samples is justified by the contribution of the research to be conducted on them to the improved understanding of an emerging risk of major public health interest, i.e., the role of early-life exposures in functional health in later life. The amount of biological samples to be collected is such as not to constitute any significant burden on the donors. Ethics approval will be sought from the local ethics committees prior to starting the fieldworks. The following procedures will be included in the research protocol to safeguard the privacy of study subjects:
- Reported study results will pertain to analyses of aggregate data. No individual’s name will be associated with any published or unpublished report of this study;
- Where personal information is used, including questionnaires and biological material it will be safety stored in secure facilities, and names will be replaced by unique study numbers, and stored separately. Primary databases and analysis files will be stored on computers with personal identifiers removed;
- Participants will be identified by a unique study number assigned by staff of the partner organizations. This unique identifier will link all basic data required for the study. The master key file linking the centre’s study numbers with personal identifiers will be maintained in each centre;
- All files containing personally identifiable information, including the master key file, will be stored in password protected computer files. Access to these files will be limited to authorized project personnel;
- Hard copy records or computer generated records containing personally identifiable information will be stored in locked cabinets in an office with limited access;
- All project personnel will be trained in the importance of confidentiality of individual records and required to sign a confidentiality agreement.
- During the project life-span information will be accessed and handled by members of the research teams only, unless specific permission has been given by the ethical committee.
Study questionnaires:
We will use standardised questionnaires and protocol applied by birth cohorts in Europe (INMA, ALSPAC, GERONIMO/REMBRANDT/MobiKids), which will ultimately make it possible for pooling data and conducting joint-analyses with European cohorts in future.